")
Eosinophilic Asthma: Why It’s Different from Regular Asthma

Asthma affects over 300 million people worldwide, but not all asthma is the same. Eosinophilic asthma is a distinct subtype driven by an overproduction of white blood cells called eosinophils that tends to be more severe, harder to control, and frequently misdiagnosed. Many patients spend years cycling through inhalers and steroids before they receive the correct diagnosis and the targeted treatment that actually works.
This guide breaks down everything you need to know what eosinophilic asthma really is, how it differs from the asthma most people know, what its symptoms look like, and what modern medicine offers in terms of treatment. Whether you've just been diagnosed or suspect your asthma isn't responding the way it should, this article is for you.
What Is Eosinophilic Asthma?
To understand eosinophilic asthma, it helps to understand the tiny cells at the center of it eosinophils. These are a type of white blood cell that the body normally uses to fight parasites and certain infections. In people with eosinophilic asthma, the immune system produces too many of these cells, and they accumulate in the airways causing chronic inflammation, swelling, and the hallmark breathing difficulties of asthma.
Eosinophilic Asthma is a type of asthma where the primary driver of airway inflammation is elevated eosinophil activity, rather than the allergic reactions (IgE-driven) that cause classic allergic asthma. This distinction matters enormously because it changes which medications are most effective — and which ones won't work at all.
How Eosinophilic Asthma Differs from Regular Asthma
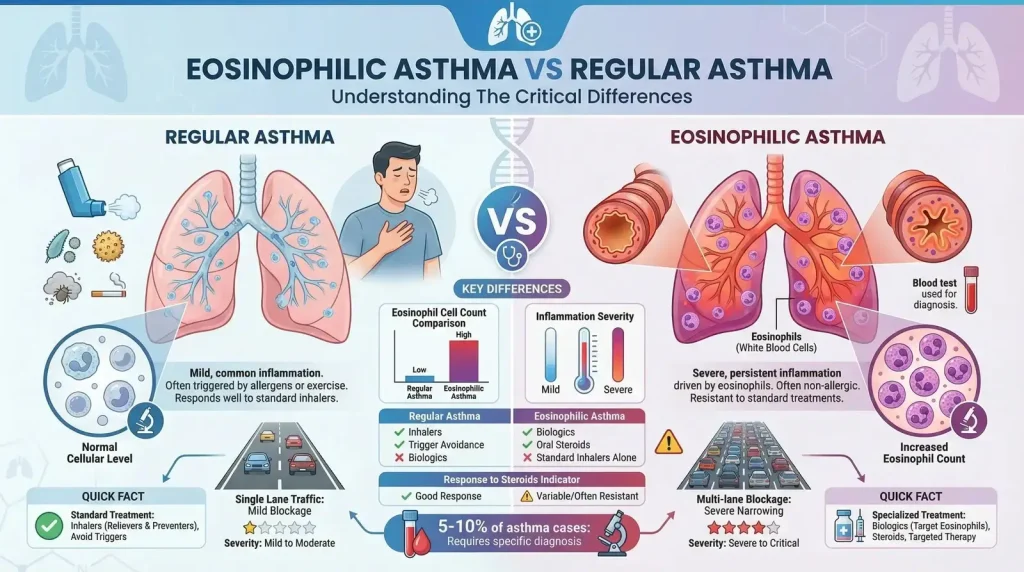
The differences between eosinophilic asthma and regular (or "classic allergic") asthma run deeper than most people realize. Here's a direct comparison
| Factor | Eosinophilic Asthma | Regular (Allergic) Asthma |
|---|---|---|
| Underlying mechanism | Eosinophil-driven airway inflammation; IL-5, IL-4, IL-13 cytokines | IgE-mediated allergic response to triggers (dust, pollen, pets) |
| Age of onset | Usually adult onset (30s–50s), often late-onset | Often begins in childhood; can persist into adulthood |
| Common triggers | NSAIDs, aspirin, exercise, stress, respiratory infections | Allergens: pollen, dust mites, pet dander, mold, smoke |
| Allergy connection | Often non-allergic (intrinsic); skin prick tests usually negative | Strongly linked to allergies (atopic); positive allergy tests |
| Severity | Frequently severe; high rate of frequent exacerbations | Ranges from mild to moderate; severe cases are less common |
| Nasal involvement | Commonly associated with nasal polyps, chronic sinusitis | May involve allergic rhinitis, but nasal polyps are less common |
| Response to steroids | Often partially resistant; may require high-dose steroids | Usually responds well to inhaled corticosteroids (ICS) |
| Biomarker | Elevated blood/sputum eosinophils; high FeNO levels | Elevated IgE; positive allergen-specific IgE |
| Best treatment | Biologic therapies (anti-IL-5, anti-IL-4/13); systemic steroids | Inhaled corticosteroids (ICS); bronchodilators; allergen avoidance |
The most clinically important difference? Standard asthma medications often fail in eosinophilic asthma. A patient using the same blue inhaler they've relied on for years may find it provides minimal relief. This is why getting the diagnosis right is not just academic — it's the difference between managing a chronic condition and suffering through repeated emergency room visits.Eosinophilic Asthma Symptoms
On the surface, eosinophilic asthma symptoms can look similar to those of regular asthma. But there are key distinguishing features that clinicians and patients alike should watch for.
Core Respiratory Symptoms
- Persistent wheezing — a high-pitched whistling sound when breathing, often worse at night or early morning
- Severe shortness of breath — often disproportionate to any identifiable trigger
- Chronic cough — particularly dry or productive, frequently unresponsive to standard cough medicines
- Chest tightness and pressure — a feeling of heaviness or constriction in the chest
- Frequent exacerbations — severe asthma attacks that require oral corticosteroids or emergency care, often multiple times per year
Associated Symptoms That Signal Eosinophilic Involvement
- Symptoms that are poorly controlled despite using prescribed inhalers correctly
- Nasal polyps — benign growths in the nasal passages causing congestion, reduced sense of smell, and sinus pain
- Chronic sinusitis and postnasal drip
- Loss of smell (anosmia) or significantly dulled sense of smell
- Fatigue and reduced exercise tolerance
Causes and Risk Factors
The exact cause of eosinophilic asthma is not fully understood, but researchers have identified several contributing factors and risk markers
Biological Causes
- Dysregulated immune response: The immune system releases excess cytokines — particularly IL-5 — which signal the bone marrow to overproduce eosinophils
- Airway epithelial dysfunction: Damage to the airway lining triggers an inflammatory cascade that draws eosinophils into the lungs
- Genetic predisposition: Certain genetic variants affecting immune regulation increase the risk, though no single gene has been identified as the sole cause
Risk Factors
- Adult onset (most cases develop in people aged 30–50, unlike childhood allergic asthma)
- Female sex (eosinophilic asthma is more common in women, particularly around hormonal changes)
- NSAID sensitivity — aspirin and ibuprofen can provoke severe attacks in a subset of patients (AERD: Aspirin-Exacerbated Respiratory Disease)
- Obesity (associated with more severe airway inflammation)
- Comorbid conditions: nasal polyps, chronic rhinosinusitis, and eosinophilic esophagitis
- Occupational exposures (certain chemicals, dust, fumes)
Importantly, many patients with eosinophilic asthma have no known allergies and no family history of atopic disease — making it harder to connect the dots without proper testing.
Is Eosinophilic Asthma an Autoimmune Disease?
This is one of the most common questions patients ask — and the answer requires some nuance. Eosinophilic asthma is not classified as an autoimmune disease in the traditional sense. Autoimmune diseases involve the immune system mistakenly attacking the body's own healthy tissues (like in rheumatoid arthritis or lupus). In eosinophilic asthma, the immune system is not attacking self-tissue per se — rather, it's mounting an exaggerated and misdirected inflammatory response in the airways.
That said, eosinophilic asthma does share some characteristics with autoimmune conditions:
- It involves immune dysregulation (the immune system behaving abnormally)
- It responds well to biologic therapies — the same class of drugs used to treat autoimmune diseases
- It can be associated with other inflammatory and autoimmune conditions (e.g., eosinophilic granulomatosis with polyangiitis, or EGPA)
- It is not caused by infection or a clear external trigger in most cases
The more accurate classification is that eosinophilic asthma is an immune-mediated inflammatory disease — driven by an overactive immune pathway rather than autoimmunity. Understanding this distinction helps explain why it requires immunomodulatory treatment rather than just conventional asthma medications.
Eosinophilic Asthma Diagnosis
Diagnosing eosinophilic asthma requires more than the standard asthma tests. A pulmonologist or allergist will typically use a combination of clinical history, blood tests, and specialized assessments.
Diagnostic Tests
- Blood eosinophil count: A simple complete blood count (CBC) with differential can reveal elevated eosinophils. A count ≥300 cells/μL is often considered significant; ≥500 cells/μL is strongly suggestive
- Sputum eosinophilia: Induced sputum analysis showing ≥3% eosinophils is a hallmark finding, though this test is not always available
- Fractional exhaled nitric oxide (FeNO): A non-invasive breath test — elevated FeNO (≥25 ppb) indicates eosinophilic airway inflammation
- Spirometry: Measures airflow obstruction; may show reduced FEV1/FVC ratio
- Bronchoscopy with bronchoalveolar lavage (BAL): In complex cases, direct sampling of airway fluid may be used to confirm eosinophilia
- Nasal endoscopy: To evaluate for associated nasal polyps
- CT scan of sinuses: To assess chronic sinusitis
Treatment Options for Eosinophilic Asthma
The good news: eosinophilic asthma treatment has been transformed in recent years by the arrival of targeted biologic therapies. Here is a comprehensive overview of available treatments
Step 1: Conventional Asthma Medications
Most patients begin with standard therapies before an eosinophilic diagnosis is confirmed:
- Inhaled corticosteroids (ICS): Fluticasone, budesonide, beclomethasone — reduce airway inflammation but are often insufficient for eosinophilic disease
- Long-acting beta-agonists (LABA): Salmeterol, formoterol — used in combination with ICS to keep airways open
- Short-acting bronchodilators (SABA): Salbutamol (albuterol) — for quick symptom relief during attacks
- Leukotriene receptor antagonists: Montelukast — may offer some benefit in eosinophilic inflammation
Step 2: Systemic Corticosteroids
Oral prednisone or prednisolone is used for exacerbations. While effective short-term, long-term systemic steroids carry serious side effects: osteoporosis, diabetes, weight gain, cataracts, adrenal suppression, and increased infection risk. For patients requiring frequent systemic steroids, this signals a need to escalate to biologic therapy.
Step 3: Biologic Therapies — The Game-Changer
Biologics are antibody-based medications that target specific molecules in the eosinophilic inflammatory pathway. They represent the biggest advance in eosinophilic asthma treatment in decades:
- Mepolizumab (Nucala): Anti-IL-5 antibody; reduces eosinophil production by blocking IL-5 signaling. Administered monthly by subcutaneous injection. Reduces exacerbations by up to 50%.
- Reslizumab (Cinqair/Cinqaero): Anti-IL-5 antibody; administered by IV infusion every 4 weeks.
- Benralizumab (Fasenra): Anti-IL-5 receptor alpha antibody; depletes eosinophils directly. Monthly injections for 3 doses, then every 8 weeks.
- Dupilumab (Dupixent): Anti-IL-4/IL-13 receptor antibody; works across multiple T2 pathways; also highly effective for nasal polyps. Every 2 weeks by injection.
- Tezepelumab (Tezspire): Anti-TSLP antibody; targets an upstream initiator of the inflammatory cascade; effective across multiple asthma phenotypes including eosinophilic.
Aspirin Desensitization
For patients with aspirin-exacerbated respiratory disease (AERD) — a subset of eosinophilic asthma — aspirin desensitization therapy performed in a specialist setting can reduce sensitivity to NSAIDs and may improve nasal polyp burden.
Bronchial Thermoplasty
A procedure that uses radiofrequency energy to reduce airway smooth muscle — considered in select severe asthma patients who don't respond to biologics.
Understanding the Eosinophilic Asthma Airway: A Visual Guide
The diagram below illustrates what happens inside the airways of someone with eosinophilic asthma compared to a healthy airway. Key elements shown include:
- Airway lumen narrowing — the open channel for airflow becomes significantly reduced
- Eosinophil accumulation — clusters of white blood cells invade the airway wall, shown in orange
- Airway wall thickening — chronic inflammation causes structural changes (remodeling)
- Excess mucus production — goblet cells overproduce mucus, further blocking airflow
- Smooth muscle hypertrophy — the muscle around the airway enlarges and tightens
Severe Eosinophilic Asthma: What Makes It Different
Severe eosinophilic asthma represents the most challenging end of the spectrum — a form of the disease that remains poorly controlled despite maximal conventional therapy, including high-dose inhaled corticosteroids plus a second controller medication.
Defining Severe Eosinophilic Asthma
By clinical definition, severe asthma is present when a patient requires Step 4–5 therapy on the GINA (Global Initiative for Asthma) treatment guidelines to prevent the asthma from becoming uncontrolled, or when the asthma remains uncontrolled despite this level of treatment. In the eosinophilic phenotype, severe means:
- Two or more severe exacerbations per year requiring systemic corticosteroids
- One or more hospitalizations or ICU admissions for asthma in the past year
- Ongoing daily oral corticosteroid dependence (prednisolone ≥10 mg/day)
- FEV1 persistently below 80% predicted despite treatment
- Significant impairment of daily activities and quality of life
The Steroid Burden Problem
One of the most serious consequences of severe eosinophilic asthma is long-term oral corticosteroid (OCS) use. While steroids suppress eosinophil activity, using them chronically causes a cascade of serious side effects — weight gain, bone thinning, diabetes, immune suppression, and adrenal insufficiency. Biologics have been shown to dramatically reduce — or even eliminate — the need for chronic steroids in many patients with severe eosinophilic asthma, which is one of the most impactful benefits of these therapies.
Eosinophilic Asthma Life Expectancy and Long-Term Outlook
However, certain risk factors can affect the long-term prognosis:
- Uncontrolled severe exacerbations: Fatal asthma attacks, while rare, are more common in patients with poorly controlled severe asthma
- Long-term OCS complications: Patients on chronic systemic steroids face elevated cardiovascular, metabolic, and bone health risks
- Fixed airflow limitation: Repeated inflammatory episodes can cause permanent airway remodeling, reducing lung function over time even between attacks
- Comorbidities: Associated conditions like nasal polyposis, EGPA, or eosinophilic esophagitis add disease burden
Frequently Asked Question
Eosinophilic asthma is a type of asthma caused by high levels of eosinophils, a kind of white blood cell that leads to inflammation in the airways. It is often more severe and harder to control than typical asthma.
Symptoms include frequent asthma attacks, shortness of breath, wheezing, chest tightness, and a persistent cough that may not respond well to standard inhalers.
Unlike typical asthma, it is not always triggered by allergies and often does not respond well to usual treatments. It tends to be more severe and may require specialized therapies.
It is linked to an overactive immune system that produces too many eosinophils, leading to airway inflammation. The exact cause is not always clear.
Doctors may use blood tests to check eosinophil levels, lung function tests, sputum analysis, and a history of frequent or severe asthma symptoms.
Treatment may include high-dose inhaled corticosteroids, oral steroids, bronchodilators, and biologic therapies that specifically target eosinophils.
There is no cure, but it can be managed effectively with the right treatment plan and regular medical care.
You should consult a doctor if your asthma symptoms are severe, frequent, or not improving with standard treatments.